
September 5, 2024
Unique Anti-obesity Drugs And Plasma Lipids Page 3
Tesofensine Wikipedia At 20 weeks, thetrial was unblinded and reached 2 years in 398 of the topics, of which 268completed the study. Topics in the sugar pill group were switched over to liraglutide2.4 mg/d at 1 year and to 3.0 mg/d at 70 weeks. From randomization to year one, topics provided the 3.0 mg dose of liraglutide lost 5.8 kg more weight thanplacebo and at year two weight reduction was 3.0 kg in excess of sugar pill [90]What is the future anti weight problems medication?
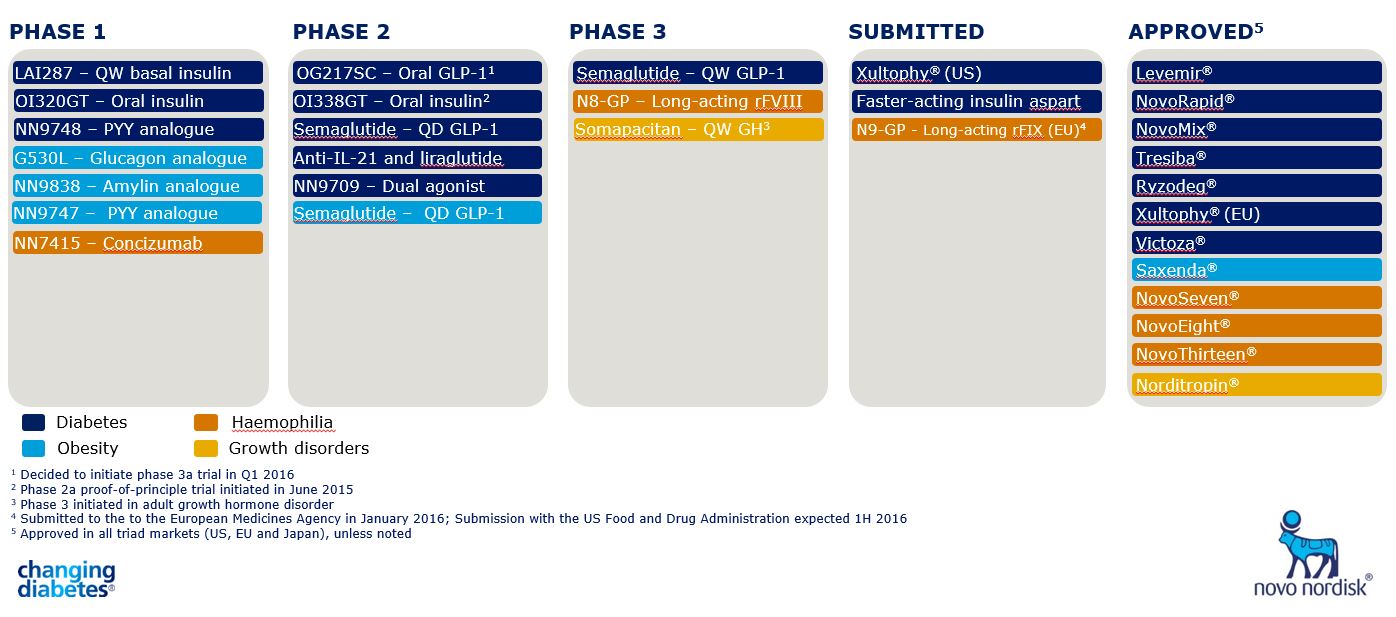
Semaglutide 2.4 mg once weekly, a subcutaneously administered GLP-1 RA accepted for weight problems treatment in 2021, leads to 15-17% mean weight-loss (WL) with evidence of cardioprotection. Oral GLP-1 RA are also under development and early data reveals similar WL efficiency to semaglutide 2.4 mg.
The Prevalence And The Medical Profile Of Metabolic Disorder In Children And Adolescents With Kind 1 Diabetes
Because of the intimate co-location of the hypothalamus, pituitary and optic chiasm, aesthetic disruption from suprasellar tumors is reasonably usual at discussion, with aesthetic disruption identified in more than 50% of clients who offer with craniopharyngioma (39 ). In addition, as a result of the co-location of the hypothalamus to structures within the cavernous sinus, craniopharyngiomas can lead to other neurological sequalae consisting of epilepsy, cranial nerve disorder and cerebrovascular events which enhance in frequency with bigger tumours (62 ). Any of these shortages either in isolation or in combination has the possible to influence on the capability to partake in exercise, and therefore raise the danger of weight problems. GLP-1R agonists potentiate glucose-induced insulin secretion (GIIS) from pancreatic β-cells, which potently boosts insulin secretion and improves insulin level of sensitivity in fat, using boosted β-cell task of GIPR. Right here, we quickly introduce new drugs under advancement with the results of professional phase 2 research studies.Activators Of Lipid And Basal Metabolism In Drug Advancement
Rest deprivation16, circadian desynchronization17, persistent stress18 and the use of anti-epileptic and psychotropic drugs19 may further drive weight gain. With an approximated heritability of ∼ 40-- 70% 20,21, the contribution of genetic variables to BMI is comparable with that reported for Tourette disorder (58-- 77%) 22, psoriasis (66%) 23, heart problem (34-- 53%) 24 or bust cancer cells (25-- 56%) 25. Positron discharge tomography (PET) was utilized to research dopaminepresynaptic transporter tenancy in the human brain after different dosages oftesofensine. Between 0.125 and lmg, there was a dose-dependent blockade ofbinding, and striatal dopamine carrier occupancy varied between 18% and 77%. in a sigmoid- shaped Emax (optimum result attributable to the drug) relationship. The sigmoid Emax version is a mathematical design that describes theconcentration- impact relationship of a medication where the curve gets more sigmoidin form as the variety of particles binding to the medication receptor increases. Therefore, throughout periods of malnourishment during which time fat mass is decreased, leptin is reduced in-turn promoting increased food consumption and fat accumulation (28 ); conversely interruption of leptin signalling advertises hyperphagia and fast weight gain (29 ). In the mediobasal hypothalamus, leptin triggers POMC whilst straight inhibiting AgRP and NPY neurons with a web impact of boosting power expenditure and decreasing food intake (30 ). Along with this, in the dorsomedial hypothalamus, leptin promotes increased energy expense with activation of brown fat which results in a decrease in body weight that is independent of food consumption (31 ). In 2013, cetilistat, a pancreatic lipase prevention, was accepted as a therapy for excessive weight in Japan, which was marketed as Oblean ® by Takeda. It has a role similarly as orlistat by inhibiting pancreatic lipase, an enzyme that hydrolyzes triglycerides into absorbable totally free fatty acids in the intestine. A 12-week, multicenter, randomized, double-blind, stage 2 clinical test was carried out in overweight clients with diabetes.- In addition, Semaglutide can be taken orally or with shot, providing a level of comfort to suit different person preferences and lifestyles.
- By resolving the underlying root causes of weight gain and excessive weight, patients can shed and keep weight off.
- These nerve cells promote feeding behavior optogenetically [8, 11], so the inhibition of these nerve cells by tesofensine might contribute to its appetite-suppressing results.
- The forward mobility was tracked making use of the rats' facility mass of the hind-limbs method and plotted as total range took a trip (cm) for 240 mins.
- The stage 2 trial contrasted lorcaserin 10mg/d, 15mg/d, 10 mg twice a day( bid) and placebo in a randomized, double-blind trial lasting 12 weeks insubjects with excessive weight (BMI 30-- 45 kg/m2) that were asked not to changetheir diet plan or exercise [71]
Social Links